5164 - Amputation not improvable by prosthesis controlled by natural knee action
DBQ: Link to Index of DBQ/Exams by Disability for DC 5164
Acronym: LLA (lower limb amputation), AKA
Definition
An amputation is the removal of a limb or a part of a limb. In this diagnostic code, the amputation has not been made functional by the use of an artificial replacement for the body part controlled by normal knee action.
{kind=link}
Etiology
The initial need for amputation may have been associated with trauma, systemic disease, cancer, bone infection or poor circulation.
Signs & Symptoms
Amputated stumps, with complications that preclude the use of a prosthesis, usually manifest: hip flexion contractures; abduction of the amputated extremity; poorly-shaped stump; infected stump; and an open wound or formation of a bony spur.
Tests
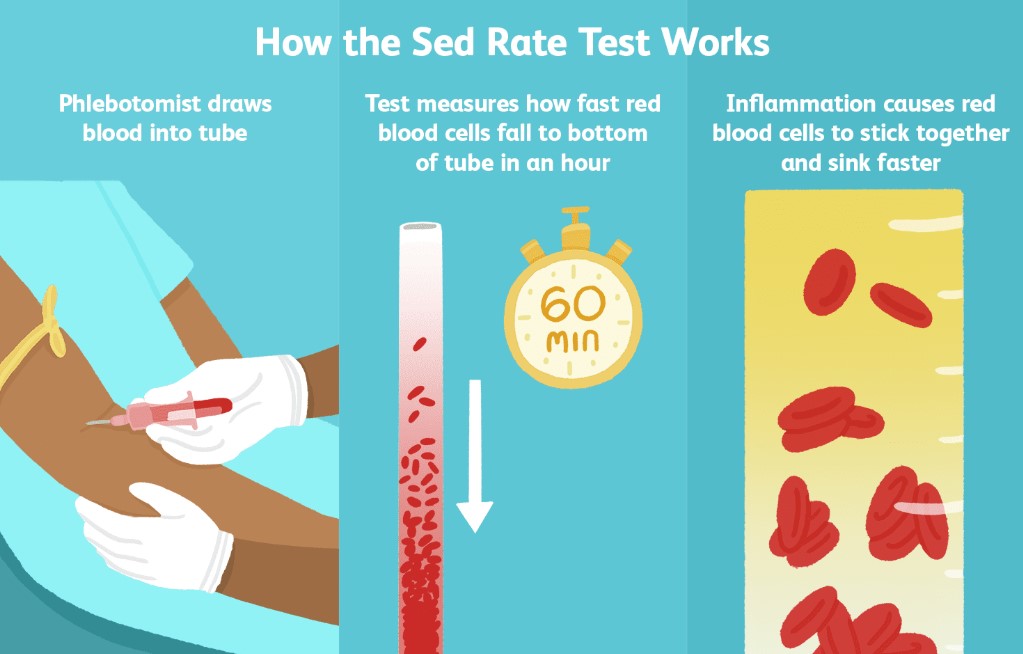
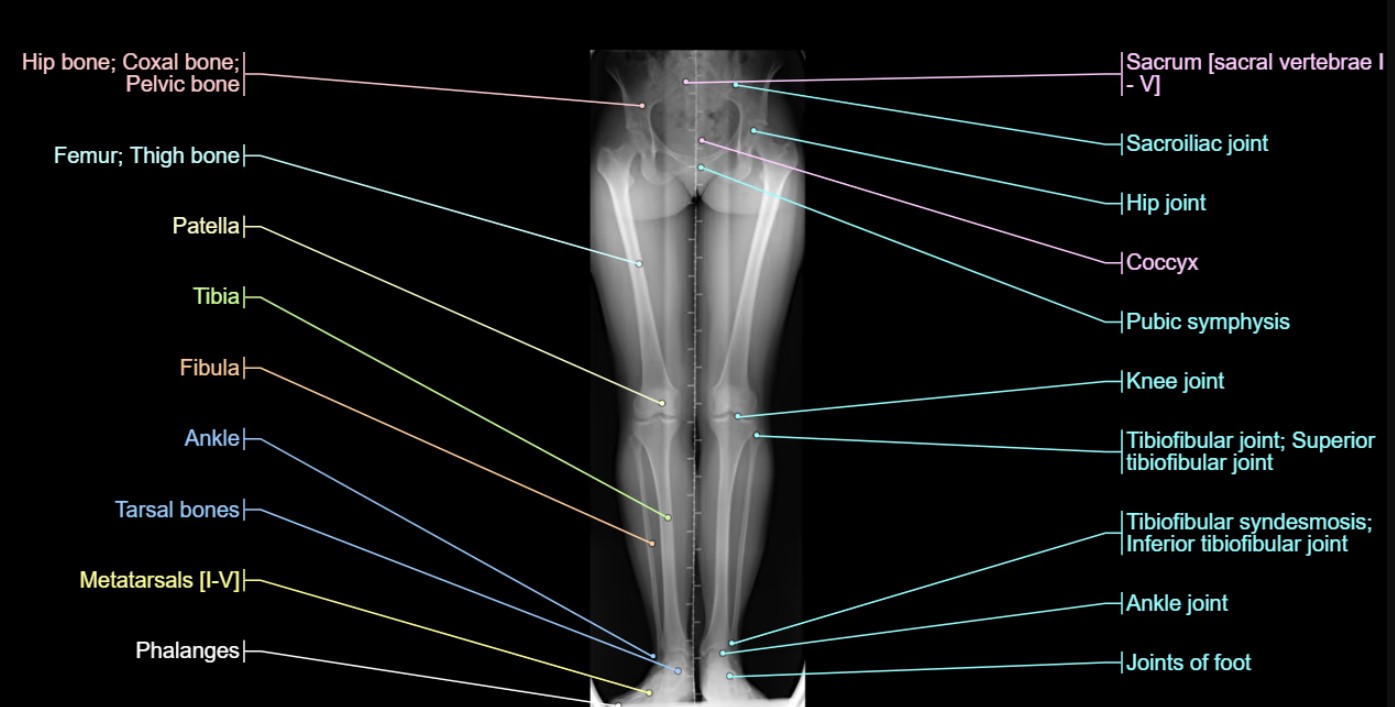
Examinations that would most likely be implemented include: wound cultures; erythrocyte sedimentation rate (ESR); computed tomography (CT) scan; x-rays; angiography; and Doppler studies.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Treatment
The focus of treatment for an amputee without the use of a prosthesis would be learning to use appropriate crutch-walking gaits. Maintenance of strength with physical therapy and exercise and use of ultrasound, corticosteroids, and analgesics for phantom limb pain are additional therapies that may be included.
{kind=link}
Residuals
-
In the aftermath of an amputation, there is an impact on body image, lifestyle, and mobility. Phantom limb pain occurs in 70% of new amputees and may require treatment. Counseling, rehabilitation, and crutch-walking with ease and safety are aspects to be considered in assisting the patient's return to normal activity.
-
When deciding expressly claimed issues, decision makers must consider entitlement to any complications that are within scope of the claim, including those identified by the rating criteria for that condition in 38 CFR Part 4. This could include but is not limited to, scars as the result of surgical intervention for a service-connected (SC) disability.
Special Considerations
-
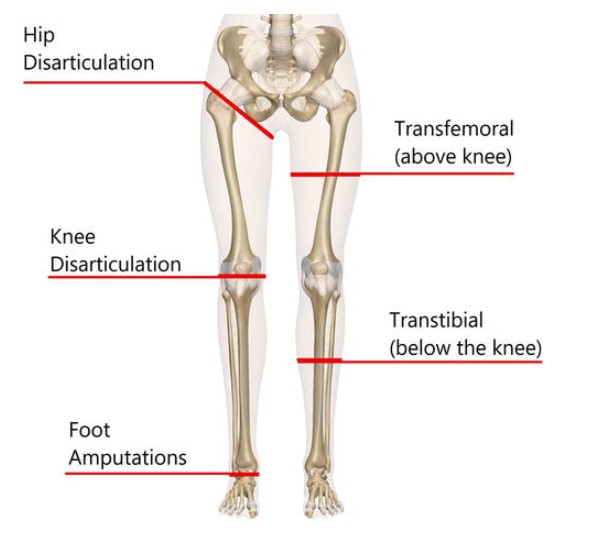
To properly rate this disability, accurate and complete descriptions of the affected extremity are necessary. Descriptions of the affected extremity should include exact place of amputation or resection, length of stump, limitations of motion, pain, weakness, carriage, gait, and posture. An occupational therapy work-up is extremely beneficial, especially when amputation of the hands or fingers is involved.
-
Consider entitlement to specially adapted housing (SAH), special home adaptation (SHA), and/or automobile or other conveyances and adaptive equipment, if otherwise in order. See 38 CFR 3.808 – Automobile or other conveyances and adaptive equipment; 38 CFR 3.809 – Specially adapted housing; 38 CFR 3.809a – Special home adaptation grants.
-
Consider entitlement to SMC under 38 CFR 3.350 as an issue in every case where there is a severe degree of disability involving the loss or loss of use of an extremity or sensory organ or any other functional loss providing entitlement to SMC.
-
38 CFR 4.30 provides for a temporary 100-percent evaluation without regard to other provisions of the rating schedule if treatment of a service-connected (SC) disability resulted in surgery necessitating at least one month convalescence surgery with severe postoperative residuals, or immobilization of at least one major joint by cast without surgery, including procedures performed at an outpatient clinic.
-
Compensation is payable under 38 U.S.C. 1160 for disabilities involving certain paired organs or extremities, one SC and the other non-service-connected (NSC), provided the NSC disability is not the result of the Veteran’s own willful misconduct.
-
A determination as to loss of use (LOU) of a hand or foot is not restricted to organic loss; it includes functional LOU as well.
-
Where an NSC cause necessitates amputation of an extremity resulting in elimination of an SC disability distal to the site of the amputation, do not sever SC for or reduce the evaluation of the SC disability.
-
With service incurred lower extremity amputation or shortening, a disabling arthritis, developing in the same extremity, or in both lower extremities, with indications of earlier, or more severe, arthritis in the injured extremity, including also arthritis of the lumbosacral joints and lumbar spine, if associated with the leg amputation or shortening, will be considered as service incurred, provided, however, that arthritis affecting joints not directly subject to strain as a result of the service incurred amputation will not be granted service connection. See 38 CFR 4.58 – Arthritis due to strain.
-
Ischemic heart disease or other cardiovascular disease, including hypertension developing in a veteran who has a service-connected amputation of one lower extremity at or above the knee or service-connected amputations of both lower extremities at or above the ankles, shall be held to be the proximate result of the service-connected amputation or amputations. See 38 CFR 3.310(c) – Disabilities that are proximately due to, or aggravated by, service-connected disease or injury.
Notes
-
Also entitled to special monthly compensation. (AMPUTATIONS: LOWER EXTREMITY)